The Perfect Match
They fit nicely together, like when you slide your hand into a perfectly snug-yet-stretchy glove.
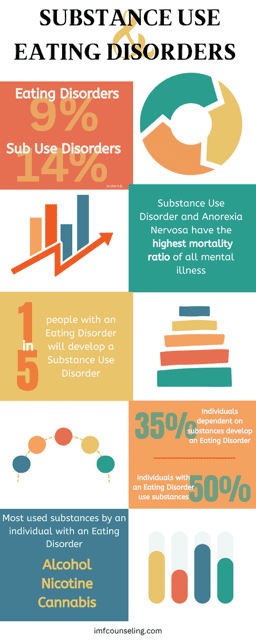
With the two highest mortality rates of all mental illness, Substance Use Disorders and Eating Disorders work incredibly well together to serve a myriad of functions in our brains and bodies. They both provide comfort, a sense of distraction, tactile sensations, companionships, and yes, a nice hit of dopamine. They are also chronic, relapsing conditions that involve compulsive behavior despite negative consequences. Both Substance Use Disorders and Eating Disorders create changes in the brain which is what lands them both in the mental illness category.
To stay out of the diagnostic weeds, I want to highlight the difference between Substance Use Disorder and substance use and Eating Disorders and disordered eating. A mental illness with the word “disorder” at the end typically means an individual has met prescriptive criteria for impairment and limited daily functioning due to a mental illness. When criteria is not met according to the Diagnostic and Statistical Manual for Mental Disorders, but negative symptoms are still present, the terminology changes a bit. In this post, we’ll be talking more generally about the similarities and differences of substance use symptoms and eating disorder/disordered eating symptoms.*
When eating disorder/disordered eating symptoms are present, someone may be struggling with patterns and behaviors of eating that feel compulsive and consuming, body image concerns, a sense of fixation on dieting, counting calories and macros, “healthy eating,” and even high levels of activity or exercise.
People who use substances often experience very similar symptoms to those with food and movement challenges: obsessive and compulsive ways of ingesting or using alcohol, illicit drugs, prescription medication, and supplements, ritualistic planning of getting high or drifting into a deep sense of relaxation, and reorganizing a daily routine or schedule to make room for substance use.
Both substance use and disordered eating follow binge-restrict patterns. Both can be used to numb or decrease negative mood or emotions OR to increase positive mood or emotions. Both trigger the same reward circuit in the brain which often keeps a person or group of people in a vicious cycle of cravings, urges, behaviors, guilt, and then, starting over.
Here’s the deal, though. Alcohol and drugs are not a biological need to sustain life. Food is. So, with all the similarities, and especially when both sets of behaviors are present at the same time, how do we work with cycles that mimic each other but deserve very different attention?
It’s not easy or simple or fast. Let’s just start there. And if you don’t want to read some of the research stats and facts, feel free to skip over the next couple paragraphs until you see a fun word: Drunkorexia.
50% of people with Eating Disorders use alcohol and drugs. 35% of people with Substance Use Disorder will develop an Eating Disorder.
- Both sets of challenges are treated most commonly through individual counseling, Intensive Outpatient Services, and even inpatient treatment.
- Where inpatient treatment for eating disorder symptoms may monitor food and liquid intake, substance use inpatient treatment will monitor drug and alcohol intake.
- Both warrant medication assistance which can be very helpful.
- Counseling in both realms involve a sort of exposure therapy for unwanted and intolerable mood and emotions, the very thing the symptoms and disorders attempt to calm and cure.
I mentioned above that these two challenges share the #1 and #2 highest mortality rate of all mental illnesses. Specifically, Anorexia Nervosa is the leader in mortality when it comes to mental disorders, followed closely by Opiate Use Disorder. Often, ingesting substances mimics ingesting food, so the felt sense to eat is often curbed by the drug which increases the risk of death when both are present. When someone is highly restricting food, perhaps even purging food, AND drinking alcohol, there is an increased risk of not just death, but sudden death, because of the instability created in one’s internal organs and bodily functioning.
Think of it like this: if you have a computer or a phone running too many programs or apps at once, sometimes there’s a crash. Our bodies and brains are the same way. If someone is not eating and using drugs, or drinking alcohol and then binge-eating and then purging, too much “programming” is attempting to happen in our bodies. Our brain doesn’t know how to return to homeostasis, a stabilized place, so all systems shut down. Substance use and disordered eating/eating disorders can be a deathly combo.
If you’re still reading, that’s incredible. That kinda fun word, “drunkorexia…” is not really that fun when you know what it is. Here are two examples of how a couple real-life conditions create chaos in our bodies and even more chaos in the treatment of the co-occurring symptoms.
- Drunkorexia: a non-medical, slang term that describes altering eating patterns to offset caloric intake from alcohol or speed up effects of alcohol.
- Cannabinoid Hyperemesis Syndrome: a medical emergency that involves repeated purging/vomiting that can often mimic symptoms of an Eating Disorder.
The latter has gotten more confusing as the legalization of marijuana has increased accessibility and consistent, daily use. Sometimes, it is even suggested to help “wake up” hunger cues in someone who is trying to recover from a lifetime of restriction. And yes, while cannabis can make someone feel hungry, it cannot correct or restructure the neurological cues that actually trigger hunger for food as a way of fueling the body. In fact, Cannabis Use Disorder is on the rise and thus presents all the challenges of working with substance use and Substance Use Disorder.**
Dieting, working out a couple times a day, drinking 5:00 p.m. wine with dinner, and smoking weed on the weekends all make sense. We all need a break, a release, an escape. And in and of themselves, these choices of ingestion and activity don’t typically pose a problem. However, when used with each other, consistently, over a period of time, and experiencing some positive shifts in mood because of it all (even if the positive shift doesn’t last long), can lead to a tricky decline.
There’s always hope, though. Feel free to send us a message to continue the conversation.
*For any type of medical and/or diagnostic inquiries, please reach out to your physician or psychiatrist, or other medical provider.
**Please discuss with your physician or medical provider if considering cannabis as part of your treatment plan.
References:
Substance Use & Substance Use Disorders
United States Addiction Statistics
Eating Disorder Statistics – National Eating Disorders Association
Substance Use Disorder defined by NIDA and SAMHSA
Cannabinoid hyperemesis syndrome masquerading as an eating disorder
Budding New Considerations about the Use of Cannabis in Eating Disorder Treatment